
Updated November 2024
RSV (Respiratory Syncytial Virus) is a common respiratory infection that most families have experienced without even knowing it. It’s so common that almost all of us and our kids have had RSV at least once before the age of two. In most cases, the symptoms of RSV are indistinguishable from the common cold. However, in rare cases, RSV can cause a serious lung infection that may require hospitalization.
This article covers the treatment and prevention of RSV and information about when it is time to see a doctor.
What Is RSV?
RSV is a common respiratory infection that most often produces mild cold symptoms, including dry cough, sneezing, low-grade fever, sore throat, congestion, and headache. People usually fully recover in 1-2 weeks.
However, in those at high risk — infants under 12 months, preterm infants, low birth weight infants, the elderly, people with underlying heart and lung disease, people with certain genetic polymorphisms, and immunocompromised people — RSV infection can result in bronchiolitis and pneumonia that could require hospitalization (1-3). Pregnant women are also at higher risk of severe RSV bronchiolitis, which may have an impact on their unborn babies (4).
SYMPTOMS OF RSV BRONCHIOLITIS & PNEUMONIA
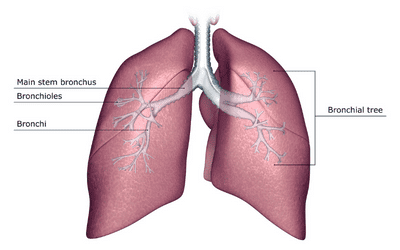
RSV bronchiolitis and pneumonia occur when RSV infects the bronchioles (small airways) and alveoli (air sacs). Severe RSV lung infection symptoms include high fever, severe cough, wheezing, rapid breathing, difficult or painful breathing, difficulty breathing while lying down, and bluish color of skin.
 In infants, severe RSV infection can include any of the above symptoms in addition to poor feeding, unusual tiredness, and irritability. Infants struggling to breathe will often breathe more quickly and shallowly and will demonstrate retractions (skin and muscles pulling inward with each breath taken).
In infants, severe RSV infection can include any of the above symptoms in addition to poor feeding, unusual tiredness, and irritability. Infants struggling to breathe will often breathe more quickly and shallowly and will demonstrate retractions (skin and muscles pulling inward with each breath taken).
WHEN TO SEE A DOCTOR FOR RSV
Seek emergency medical care if the person with RSV has a high fever, difficulty breathing, and/or bluish color to the skin, lips, or nail beds.
COMPLICATIONS OF RSV BRONCHIOLITIS AND PNEUMONIA
RSV bronchiolitis and pneumonia may cause difficulty breathing to the degree that hospitalization is required. At the hospital, IV fluids may be necessary to prevent dehydration and humidified oxygen may be administered to keep blood oxygen levels high. In rare cases, mechanical ventilation could be needed (5).
There is some evidence that infants and children who get severe bronchiolitis as a result of RSV infection may be at greater risk for developing asthma later in life, however current consensus is that RSV infection does not increase risk of asthma significantly (5,6). Additionally, there’s evidence RSV infection during pregnancy is associated with greater risk for some types of immune issues and lung dysfunction in the child (7).
People with RSV may be at greater risk for a viral or bacterial co-infection with pathogens like influenza, SARS-CoV-2 (Covid-19), and others (8). Co-infections are infections that occur at the same time. If co-infection occurs, symptoms tend to be more severe (9).
Read more about bronchiolitis & pneumonia: Bronchitis, Bronchiolitis, Pneumonia, & Mycoplasma Pneumonia – Dr. Green Mom
Natural Treatment For RSV
Natural treatment for RSV includes keeping the airways clear and hydrated, preventing dehydration, and providing supportive comfort through natural remedies. Natural remedies are intended to support the body and provide temporary relief of symptoms; it is the body’s own immune defenses that resolve the infection.
1. KEEP AIRWAYS CLEAR AND HYDRATED
Keeping airways clear and hydrated is an important part of RSV management, especially for small babies. Because babies can’t clear mucus from their nostrils, manually removing mucus is necessary. I prefer a nasal aspirator for babies, but the NoseFrida or a simple nasal bulb works well, too.
Saline or xylitol drops can be administered to loosen mucus.
Steam inhalation is a common treatment for RSV and other respiratory infections because it soothes and hydrates the respiratory tissues.
For more information about how to set up a steam inhalation for your kids and which herbs and essential oils are helpful, see this article: Botanical Steam Inhalation To Reduce Congestion & Soothe Coughs – Dr. Green Mom.
Note: Many people recommend cool mist inhalation for RSV and other coughs and colds. I hesitate to recommend it because even the most well-maintained humidifiers are often home to mold and other pathogens that may cause more harm than good (10). If choosing to use a humidifier, make sure that it is easy to clean and is well-maintained.
2. PREVENT DEHYDRATION
Preventing dehydration is important any time a child has an infection. Soothing teas with antiviral spices are a good option as are chicken soup and congee. You can also rely on homemade electrolyte drinks, coconut water, and breast milk for hydration.
Signs of dehydration to watch for include decreased urine output and fewer wet diapers, dry lips and mouth, decreased tears when crying, dizziness, sunken eyes, and sunken fontanelles in babies.
Read more: Signs of Dehydration & Homemade Electrolyte Drink Recipe – Dr. Green Mom
3. FEVER MANAGEMENT & COMFORT
Fevers are a normal part of childhood upper respiratory infections. When looking after feverish kiddos, the symptoms are more important than the number on the thermometer. If a child is quietly playing and acting like a slightly more subdued version of their usual self, I tend not to worry even when the fever is high. This is because fevers are part of the body’s natural defense system and fevers (less than 104F or 40C) are associated with faster and better recovery from infections (11).
Traditional herbal fever remedies are helpful for immune system support and for helping the body feel cooler and more comfortable without actually suppressing the fever.
Conventional fever reducers like acetaminophen and ibuprofen will suppress a fever and lower body temperature. I find them most helpful when uncomfortable body pain accompanies fever, when the fever is interfering with sleep, and/or when the fever is high (over 104F or 40C).
Read more about natural strategies for fever comfort & relief:
Fevers 101: Benefits, Home Care Strategies, & When to Medicate
The Wet Sock Treatment: A Home Remedy For Colds & Flus
4. COUGH TREATMENT
Sometimes a mild cough can accompany RSV infection. There are many natural ways to soothe a cough, including essential oil chest rubs, botanical steam inhalations, and herbal teas with honey. Read more: Natural Treatment for Coughs – Dr. Green Mom
I prefer to avoid over-the-counter cough suppressants when possible because coughing is an important reflex for clearing the lungs. However, I do use OTC cough suppressants when coughing interferes with sleep, causes exhaustion, and/or leads to vomiting.
OTC cough suppressants aren’t recommended for children under 4 years old; they may be used for children aged 4-6 if advised by a doctor. Children 6 and up may use OTC cough suppressants as directed on the label.
5. IMMUNE ESSENTIAL NUTRIENTS
Natural treatment of any viral infection usually involves supporting nutrient stores so that the immune system can respond to illness. Nutrients required for a well-functioning immune system include: vitamins A, B2, B6, B12, C, D, E, folate, iron, selenium, and zinc (12-14). In general, nutrients are ideally sourced from whole foods, but supplementation may be helpful in maintaining levels of these nutrients if the diet is lacking. Read more: Is Getting Nutrients From Food Better Than Taking a Supplement?
Better Vitamin D status in newborns is associated with lower risk of RSV bronchiolitis (13). This means that vitamin D supplementation during pregnancy and in infants postpartum could be an important preventative strategy, however, this strategy has yet to be fully researched.
Early research also shows that zinc may decrease the amount of RSV in the lungs, but again these results are still preliminary – we do not yet know if zinc supplementation has any effect on RSV in terms of treatment or prevention (14).
6. BOTANICALS & HOMEOPATHIC REMEDIES FOR SYMPTOM SUPPORT
Natural remedies are helpful in mild cases of RSV for temporary relief of minor upper respiratory symptoms. Take a look at the following articles for ideas:
- How to Make An Onion Poultice: A Natural Cough Remedy for Chest Congestion
- Natural Treatment for Coughs
- Botanical Steam Inhalation to Reduce Congestion & Soothe Coughs
- The Wet Sock Treatment: A Home Remedy for Colds & Flus
- Winter Immune Support for All Ages
THINGS TO KEEP IN MIND WHEN CHOOSING NATURAL REMEDIES
When combining natural remedies, it is important to check the different herbs and nutrients in each supplement to ensure that you aren’t inadvertently getting double doses. Herbs may interact with OTC and prescription medications – don’t use them together unless advised by a doctor or pharmacist.
Homeopathic remedies don’t interact with each other, but care must be taken with appropriate dosing, especially for babies. Choose remedies that are 6C, 30C, or 200C. Avoid remedies marked with an “X” unless prescribed by a qualified healthcare provider. Remedies indicated with an “X” are less dilute than those indicated with a “C” and may include toxic levels of some herbs. Learn more about homeopathic medicine here: How To Use Homeopathic Remedies – A Quick-Start Guide For Families
Conventional Treatment of RSV
At present, there is no approved conventional treatment for RSV. Supportive care is recommended. This includes staying hydrated, resting with the head elevated, saline nasal drops, nasal suction, and fever management medication.
Bronchodilators and steroid inhalers have been evaluated as potential treatments for RSV, but haven’t been found effective. Hospital treatment of severe RSV includes IV fluids, humidified oxygen, and rarely mechanical ventilation (5).
These articles may be helpful:
- How to Use a Saline Sinus Rinse for Stuffy Noses
- Signs of Dehydration in Kids & Infants. Plus Dr. Green Mom’s Homemade Electrolyte Drink Recipe
Preventing RSV: Steps You Can Take
Preventing RSV largely involves the same strategies used to avoid other contagious upper respiratory infections. Key steps include:
- Practicing good hygiene: Wash hands frequently and avoid touching your face.
- Limiting close contact: Especially with people who may be sick.
- Prioritizing sleep: A well-rested body supports a stronger immune system.
- Following an anti-inflammatory diet & lifestyle: Nutrient-dense foods like fruits, vegetables, and omega-3-rich options support immune health.
When it comes to protecting your infant, additional steps to follow include:
- Require everyone have clean hands: Wash hands before touching your baby and require others to do the same. Get your whole family into the habit of washing hands as soon as you enter the home.
- Keep your infant away from smoke: Do not let anyone smoke in your home or around your baby. If someone close to you smokes, ensure they are in clean (smoke-free) clothes and have clean hands before touching your baby.
- Wash everything frequently: This includes toys, clothes, bedding, and household surfaces.
- Reduce germ exposure: Keep your baby away from crowds, people with upper respiratory symptoms, and young children as much as possible.
Immunization Options for RSV
There are two immunization options to help reduce the risk of severe RSV for infants.
- Abrysvo RSV Vaccine
The Abrysvo vaccine is approved for use during pregnancy to help protect newborns from RSV in their first months of life. By passing immunity from the pregnant parent to the baby, this vaccine can reduce the risk of severe RSV illness. - Beyfortus (Nirsevimab) Monoclonal Antibody
Beyfortus is a monoclonal antibody recommended for all infants in their first RSV season. This preventive option provides direct immune support to help guard against RSV infection.
For babies at higher risk, such as those born prematurely or with certain medical conditions, Palivizumab, another monoclonal antibody, may still be used.
To learn more about these immunization options and how they might fit into your family’s RSV prevention plan, visit our comprehensive blog article on RSV immunization options.
Vitamin D and RSV
As mentioned above, low vitamin D levels in newborns are associated with more severe RSV infections. Maintaining healthy prenatal and postnatal vitamin D levels is important for optimal immune function, so be sure to discuss vitamin D supplementation with your healthcare provider. Read more here: Vitamin D Supplementation for Babies
Breastfeeding and RSV
Studies have shown that infants who are breastfed have lower rates of RSV-associated lower respiratory infection. In particular, the risk of RSV bronchiolitis is significantly lower among breastfed infants compared to those who were never breastfed.
 For instance, a large study in Italy found that the risk of RSV bronchiolitis was 7% in never breastfed infants compared to 3.9% in those who were ever breastfed. Note: The ever breastfed infants in this study included infants who were partially and/or fully breastfed and who received maternal and/or donor milk.
For instance, a large study in Italy found that the risk of RSV bronchiolitis was 7% in never breastfed infants compared to 3.9% in those who were ever breastfed. Note: The ever breastfed infants in this study included infants who were partially and/or fully breastfed and who received maternal and/or donor milk.
Breastfeeding is linked to a reduced need for hospitalization due to RSV-related complications. Multiple studies indicate that breastfed infants have a lower risk of severe RSV infections requiring hospital admission. For example, one Italian study found that breastfed infants under 12 months had a hospitalization rate of 4% versus over 8% for non-breastfed infants – a 50% reduction (15).
Research about the exact benefit of breastfeeding on RSV outcomes is highly variable. For a deeper dive into this topic, check out this systematic review published by the British Medical Journal: Impact of breastfeeding on the incidence and severity of respiratory syncytial virus (RSV)-associated acute lower respiratory infections in infants: a systematic review highlighting the global relevance of primary prevention
Summary
RSV (Respiratory Syncytial Virus) is a common virus that usually causes a mild upper respiratory infection. Usually, the symptoms of RSV are mild and similar to the common cold. In rare cases, RSV can be serious and require hospitalization, so it is important to be aware of warning signs and know when to see medical help. Conventional and natural treatments for minor RSV infections involve supportive care that allows the immune system to fight off the infection while providing comfort and temporary relief of symptoms.
Breastfeeding, good hygiene, supporting overall good health and nutrition, avoiding germs, and staying away from secondhand smoke remain important steps to help reduce the risk of serious RSV infections. Two new RSV immunization options are available to add further protection for infants. Read more about them here: RSV Immunization: What Parents Should Know About Protecting Newborns.
References:
- Córdova-Dávalos, L. E., Hernández-Mercado, A., Barrón-García, C. B., Rojas-Martínez, A., Jiménez, M., Salinas, E., & Cervantes-García, D. (2022). Impact of genetic polymorphisms related to innate immune response on respiratory syncytial virus infection in children. Virus genes, 58(6), 501–514. https://doi.org/10.1007/s11262-022-01932-6
- Nguyen-Van-Tam, J. S., O’Leary, M., Martin, E. T., Heijnen, E., Callendret, B., Fleischhackl, R., Comeaux, C., Tran, T. M. P., & Weber, K. (2022). Burden of respiratory syncytial virus infection in older and high-risk adults: a systematic review and meta-analysis of the evidence from developed countries. European respiratory review : an official journal of the European Respiratory Society, 31(166), 220105. https://doi.org/10.1183/16000617.0105-2022
- Shi, T., Balsells, E., Wastnedge, E., Singleton, R., Rasmussen, Z. A., Zar, H. J., Rath, B. A., Madhi, S. A., Campbell, S., Vaccari, L. C., Bulkow, L. R., Thomas, E. D., Barnett, W., Hoppe, C., Campbell, H., & Nair, H. (2015). Risk factors for respiratory syncytial virus associated with acute lower respiratory infection in children under five years: Systematic review and meta-analysis. Journal of global health, 5(2), 020416. https://doi.org/10.7189/jogh.05.020416
- Wheeler, S. M., Dotters-Katz, S., Heine, R. P., Grotegut, C. A., & Swamy, G. K. (2015). Maternal Effects of Respiratory Syncytial Virus Infection during Pregnancy. Emerging infectious diseases, 21(11), 1951–1955. https://doi.org/10.3201/eid2111.150497
- Jain H, Schweitzer JW, Justice NA. Respiratory Syncytial Virus Infection in Children. [Updated 2023 Jun 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. https://www.ncbi.nlm.nih.gov/books/NBK459215/
- Norlander, A. E., & Peebles, R. S., Jr. (2020). Innate Type 2 Responses to Respiratory Syncytial Virus Infection. Viruses, 12(5), 521. https://doi.org/10.3390/v12050521
- Manti, S., Leonardi, S., Rezaee, F., Harford, T. J., Perez, M. K., & Piedimonte, G. (2022). Effects of Vertical Transmission of Respiratory Viruses to the Offspring. Frontiers in immunology, 13, 853009. https://doi.org/10.3389/fimmu.2022.853009
- Swets, M. C., Russell, C. D., Harrison, E. M., Docherty, A. B., Lone, N., Girvan, M., Hardwick, H. E., ISARIC4C Investigators, Visser, L. G., Openshaw, P. J. M., Groeneveld, G. H., Semple, M. G., & Baillie, J. K. (2022). SARS-CoV-2 co-infection with influenza viruses, respiratory syncytial virus, or adenoviruses. Lancet (London, England), 399(10334), 1463–1464. https://doi.org/10.1016/S0140-6736(22)00383-X
- Le-Corre, N., Pérez, R., Vizcaya, C., Martínez-Valdebenito, C., López, T., Monge, M., Alarcón, R., Moller, F., Martínez, M. T., Massardo, J. M., & Ferrés, M. (2021). Relevance of codetection of respiratory viruses in the severity of acute respiratory infection in hospitalized children. Relevancia de la co-detección de virus respiratorios en la severidad de la infección respiratoria aguda en niños hospitalizados. Andes pediatrica : revista Chilena de pediatria, 92(3), 349–358. https://doi.org/10.32641/andespediatr.v92i3.1756
- Shimoda, M., Morimoto, K., Tanaka, Y., Ken, O., & Yoshimori, K. (2020). Humidifier lung induced by endotoxin and various pathogens: Characteristic differences from other phenotypes of hypersensitivity pneumonitis. Respiratory medicine case reports, 31, 101267. https://doi.org/10.1016/j.rmcr.2020.101267
- Walter, E. J., Hanna-Jumma, S., Carraretto, M., & Forni, L. (2016). The pathophysiological basis and consequences of fever. Critical care (London, England), 20(1), 200. https://doi.org/10.1186/s13054-016-1375-5
- Maggini, S., Pierre, A., & Calder, P. C. (2018). Immune Function and Micronutrient Requirements Change over the Life Course. Nutrients, 10(10), 1531. https://doi.org/10.3390/nu10101531
- Maxwell, C. S., Carbone, E. T., & Wood, R. J. (2012). Better newborn vitamin D status lowers RSV-associated bronchiolitis in infants. Nutrition reviews, 70(9), 548–552. https://doi.org/10.1111/j.1753-4887.2012.00517.x
- Sadeghsoltani, F., Mohammadzadeh, I., Safari, M. M., Hassanpour, P., Izadpanah, M., Qujeq, D., Moein, S., & Vaghari-Tabari, M. (2022). Zinc and Respiratory Viral Infections: Important Trace Element in Anti-viral Response and Immune Regulation. Biological trace element research, 200(6), 2556–2571. https://doi.org/10.1007/s12011-021-02859-z
- Mineva GM, Purtill H, Dunne CP, et alImpact of breastfeeding on the incidence and severity of respiratory syncytial virus (RSV)-associated acute lower respiratory infections in infants: a systematic review highlighting the global relevance of primary preventionBMJ Global Health 2023;8:e009693.
Supporting Research:
Norlander, A. E., & Peebles, R. S., Jr. (2020). Innate Type 2 Responses to Respiratory Syncytial Virus Infection. Viruses, 12(5), 521. https://doi.org/10.3390/v12050521
Córdova-Dávalos, L. E., Hernández-Mercado, A., Barrón-García, C. B., Rojas-Martínez, A., Jiménez, M., Salinas, E., & Cervantes-García, D. (2022). Impact of genetic polymorphisms related to innate immune response on respiratory syncytial virus infection in children. Virus genes, 1–14. Advance online publication. https://doi.org/10.1007/s11262-022-01932-6
Borchers, A. T., Chang, C., Gershwin, M. E., & Gershwin, L. J. (2013). Respiratory syncytial virus–a comprehensive review. Clinical reviews in allergy & immunology, 45(3), 331–379 https://doi.org/10.1007/s12016-013-8368-9
Efstathiou, C., Abidi, S. H., Harker, J., & Stevenson, N. J. (2020). Revisiting respiratory syncytial virus’s interaction with host immunity, towards novel therapeutics. Cellular and molecular life sciences : CMLS, 77(24), 5045–5058. https://doi.org/10.1007/s00018-020-03557-0
Haddadin, Z., Rankin, D. A., Lipworth, L., Suh, M., McHenry, R., Blozinski, A., George, S. S., Fernandez, K. N., Varjabedian, R., Spieker, A. J., Shepard, D. S., & Halasa, N. B. (2021). Respiratory Virus Surveillance in Infants across Different Clinical Settings. The Journal of pediatrics, 234, 164–171.e2. https://doi.org/10.1016/j.jpeds.2021.03.036
Manti, S., Leonardi, S., Rezaee, F., Harford, T. J., Perez, M. K., & Piedimonte, G. (2022). Effects of Vertical Transmission of Respiratory Viruses to the Offspring. Frontiers in immunology, 13, 853009. https://doi.org/10.3389/fimmu.2022.853009
Swets, M. C., Russell, C. D., Harrison, E. M., Docherty, A. B., Lone, N., Girvan, M., Hardwick, H. E., ISARIC4C Investigators, Visser, L. G., Openshaw, P., Groeneveld, G. H., Semple, M. G., & Baillie, J. K. (2022). SARS-CoV-2 co-infection with influenza viruses, respiratory syncytial virus, or adenoviruses. Lancet (London, England), 399(10334), 1463–1464. https://doi.org/10.1016/S0140-6736(22)00383-X
Wheeler SM, Dotters-Katz S, Heine RP, Grotegut CA, Swamy GK. Maternal Effects of Respiratory Syncytial Virus Infection during Pregnancy. Emerg Infect Dis. 2015 Nov;21(11):1951-5. doi: 10.3201/eid2111.150497. PMID: 26485575; PMCID: PMC4622246
Walter EJ, Hanna-Jumma S, Carraretto M, Forni L. The pathophysiological basis and consequences of fever. Crit Care. 2016 Jul 14;20(1):200. doi: 10.1186/s13054-016-1375-5. PMID: 27411542; PMCID: PMC4944485
Sadeghsoltani, F., Mohammadzadeh, I., Safari, M. M., Hassanpour, P., Izadpanah, M., Qujeq, D., Moein, S., & Vaghari-Tabari, M. (2022). Zinc and Respiratory Viral Infections: Important Trace Element in Anti-viral Response and Immune Regulation. Biological trace element research, 200(6), 2556–2571.https://doi.org/10.1007/s12011-021-02859-z
Suara, R. O., & Crowe, J. E., Jr (2004). Effect of zinc salts on respiratory syncytial virus replication. Antimicrobial agents and chemotherapy, 48(3), 783–790. https://doi.org/10.1128/AAC.48.3.783-790.2004
Kawasaki, Y., Hosoya, M., Katayose, M., & Suzuki, H. (1999). Kansenshogaku zasshi. The Journal of the Japanese Association for Infectious Diseases, 73(2), 104–109.https://doi.org/10.11150/kansenshogakuzasshi1970.73.104
Quinlan, K. P., & Hayani, K. C. (1996). Vitamin A and respiratory syncytial virus infection. Serum levels and supplementation trial. Archives of pediatrics & adolescent medicine, 150(1), 25–30.https://doi.org/10.1001/archpedi.1996.02170260029004
Maxwell, C. S., Carbone, E. T., & Wood, R. J. (2012). Better newborn vitamin D status lowers RSV-associated bronchiolitis in infants. Nutrition reviews, 70(9), 548–552. https://doi.org/10.1111/j.1753-4887.2012.00517.x
Ji, J. J., Sun, Q. M., Nie, D. Y., Wang, Q., Zhang, H., Qin, F. F., Wang, Q. S., Lu, S. F., Pang, G. M., & Lu, Z. G. (2021). Probiotics protect against RSV infection by modulating the microbiota-alveolar-macrophage axis. Acta pharmacologica Sinica, 42(10), 1630–1641. https://doi.org/10.1038/s41401-020-00573-5
Luoto, R., Ruuskanen, O., Waris, M., Kalliomäki, M., Salminen, S., & Isolauri, E. (2014). Prebiotic and probiotic supplementation prevents rhinovirus infections in preterm infants: a randomized, placebo-controlled trial. The Journal of allergy and clinical immunology, 133(2), 405–413. https://doi.org/10.1016/j.jaci.2013.08.020
Fonseca, W., Malinczak, C. A., Fujimura, K., Li, D., McCauley, K., Li, J., Best, S., Zhu, D., Rasky, A. J., Johnson, C. C., Bermick, J., Zoratti, E. M., Ownby, D., Lynch, S. V., Lukacs, N. W., & Ptaschinski, C. (2021). Maternal gut microbiome regulates immunity to RSV infection in offspring. The Journal of experimental medicine, 218(11), e20210235. https://doi.org/10.1084/jem.20210235
Du, T., Lei, A., Zhang, N., & Zhu, C. (2022). The Beneficial Role of Probiotic Lactobacillus in Respiratory Diseases. Frontiers in immunology, 13, 908010. https://doi.org/10.3389/fimmu.2022.908010
Shin, H. B., Choi, M. S., Yi, C. M., Lee, J., Kim, N. J., & Inn, K. S. (2015). Inhibition of respiratory syncytial virus replication and virus-induced p38 kinase activity by berberine. International immunopharmacology, 27(1), 65–68. https://doi.org/10.1016/j.intimp.2015.04.045
Zhang, T., Li, J., Shi, L., Feng, S., & Li, F. (2022). Anti-RSV activities of chicoric acid from Echinacea purpurea in vitro. Minerva surgery, 77(1), 78–80. https://doi.org/10.23736/S2724-5691.21.08925-5
Wang, X. Q., Li, H. Y., Liu, X. Y., Zhang, F. M., Li, X., Piao, Y. A., Xie, Z. P., Chen, Z. H., & Li, X. (2006). Zhong yao cai = Zhongyaocai = Journal of Chinese medicinal materials, 29(7), 692–694.
Morris, D., Ansar, M., Speshock, J., Ivanciuc, T., Qu, Y., Casola, A., & Garofalo, R. (2019). Antiviral and Immunomodulatory Activity of Silver Nanoparticles in Experimental RSV Infection. Viruses, 11(8), 732.https://doi.org/10.3390/v11080732
Le-Corre, N., Pérez, R., Vizcaya, C., Martínez-Valdebenito, C., López, T., Monge, M., Alarcón, R., Moller, F., Martínez, M. T., Massardo, J. M., & Ferrés, M. (2021). Relevance of codetection of respiratory viruses in the severity of acute respiratory infection in hospitalized children. Relevancia de la co-detección de virus respiratorios en la severidad de la infección respiratoria aguda en niños hospitalizados. Andes pediatrica : revista Chilena de pediatria, 92(3), 349–358. https://doi.org/10.32641/andespediatr.v92i3.1756
Swets, M. C., Russell, C. D., Harrison, E. M., Docherty, A. B., Lone, N., Girvan, M., Hardwick, H. E., ISARIC4C Investigators, Visser, L. G., Openshaw, P., Groeneveld, G. H., Semple, M. G., & Baillie, J. K. (2022). SARS-CoV-2 co-infection with influenza viruses, respiratory syncytial virus, or adenoviruses. Lancet (London, England), 399(10334), 1463–1464. https://doi.org/10.1016/S0140-6736(22)00383-X
Castagno, E., Raffaldi, I., Del Monte, F., Garazzino, S., & Bondone, C. (2022). New epidemiological trends of respiratory syncytial virus bronchiolitis during COVID-19 pandemic. World journal of pediatrics : WJP, 1–3. Advance online publication. https://doi.org/10.1007/s12519-022-00623-4
Di Mattia, G., Nenna, R., Mancino, E., Rizzo, V., Pierangeli, A., Villani, A., & Midulla, F. (2021). During the COVID-19 pandemic where has respiratory syncytial virus gone?. Pediatric pulmonology, 56(10), 3106–3109.https://doi.org/10.1002/ppul.25582
Fourgeaud, J., Toubiana, J., Chappuy, H., Delacourt, C., Moulin, F., Parize, P., Scemla, A., Abid, H., Leruez-Ville, M., & Frange, P. (2021). Impact of public health measures on the post-COVID-19 respiratory syncytial virus epidemics in France. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology, 40(11), 2389–2395. https://doi.org/10.1007/s10096-021-04323-1
Reyes Domínguez, A. I., Pavlovic Nesic, S., Urquía Martí, L., Pérez González, M., Reyes Suárez, D., & García-Muñoz Rodrigo, F. (2022). Effects of public health measures during the SARS-CoV-2 pandemic on the winter respiratory syncytial virus epidemic: An interrupted time series analysis. Paediatric and perinatal epidemiology, 36(3), 329–336. https://doi.org/10.1111/ppe.12829
Alrayes, T., Wait, A., Spencer, P., Merolla, D. M., Lampe, K., Salimnia, H., & Kannikeswaran, N. (2022). Features of an Atypical RSV Surge During the COVID-19 Pandemic. Clinical pediatrics, 99228221124677. Advance online publication. https://doi.org/10.1177/00099228221124677
Castagno, E., Raffaldi, I., Del Monte, F., Garazzino, S., & Bondone, C. (2022). New epidemiological trends of respiratory syncytial virus bronchiolitis during COVID-19 pandemic. World journal of pediatrics : WJP, 1–3. Advance online publication. https://doi.org/10.1007/s12519-022-00623-4
Bermúdez Barrezueta, L., Matías Del Pozo, V., López-Casillas, P., Brezmes Raposo, M., Gutiérrez Zamorano, M., & Pino Vázquez, M. A. (2022). Variation in the seasonality of the respiratory syncytial virus during the COVID-19 pandemic. Infection, 50(4), 1001–1005. https://doi.org/10.1007/s15010-022-01794-y
Wei J. S. (2020). How lethal is SARS-CoV-2 pneumonia when compared with respiratory syncytial virus and influenza in young children?. Australian journal of general practice, 49(10), 683–686. https://doi.org/10.31128/AJGP-04-20-5357
Williams, T. C., Sinha, I., Barr, I. G., & Zambon, M. (2021). Transmission of paediatric respiratory syncytial virus and influenza in the wake of the COVID-19 pandemic. Euro surveillance : bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin, 26(29), 2100186. https://doi.org/10.2807/1560-7917.ES.2021.26.29.2100186
Binns, E., Koenraads, M., Hristeva, L., Flamant, A., Baier-Grabner, S., Loi, M., Lempainen, J., Osterheld, E., Ramly, B., Chakakala-Chaziya, J., Enaganthi, N., Simó Nebot, S., & Buonsenso, D. (2022). Influenza and respiratory syncytial virus during the COVID-19 pandemic: Time for a new paradigm?. Pediatric pulmonology, 57(1), 38–42. https://doi.org/10.1002/ppul.25719
Piret, J., & Boivin, G. (2022). Viral Interference between Respiratory Viruses. Emerging infectious diseases, 28(2), 273–281. https://doi.org/10.3201/eid2802.211727
Mosscrop, L. G., Williams, T. C., & Tregoning, J. S. (2022). Respiratory syncytial virus after the SARS-CoV-2 pandemic – what next?. Nature reviews. Immunology, 22(10), 589–590. https://doi.org/10.1038/s41577-022-00764-7







